
The decision to premedicate a patient is no longer a simple clinical checkbox; it’s a high-stakes workflow that directly impacts your practice’s medico-legal standing. Since the 2021 AHA scientific statement removed clindamycin from the standard of care due to risks of C. difficile infection, many teams have struggled to reconcile outdated habits with current evidence-based requirements. You likely feel the daily friction of managing patients who forget their dose or orthopedic surgeons who insist on protocols that contradict the 2015 ADA joint replacement guidelines.
This guide helps you master the clinical, legal, and communication protocols required to manage prophylaxis safely and efficiently. Why it’s critical: failing to document the rationale for antibiotic use or the decision to withhold it can expose your practice to significant liability. You will gain a clear understanding of the April 2026 antibiotic regimens, learn how to standardize your documentation, and discover how to use automated communication to ensure patient compliance without adding friction to your busy day.
Key Takeaways
- Identify high-risk patients with precision using the latest AHA and ADA clinical guidelines for cardiac conditions and prosthetic joints.
- Protect your practice from medico-legal liability by learning why the decision to premedicate must be backed by standardized, vetted documentation.
- Reduce the risk of procedure day cancellations by addressing the psychology of patient forgetfulness through automated digital communication.
- Discover how to integrate digital consent and medication verification into your workflow using a library of over 80 vetted templates.
- Transition from chaotic manual tracking to a frictionless, paperless system that ensures the standard of care is met for every patient, every time.
What Does it Mean to Premedicate? Definition and Dental Context
In the high-pressure environment of a modern operatory, the directive to premedicate carries significant clinical and legal weight. At its core, premedication is the administration of targeted pharmaceuticals, usually antibiotics or anxiolytics, before a dental procedure begins. While the term is often used as a shorthand for Dental antibiotic prophylaxis, its application in dentistry serves two distinct masters: infection prevention and patient management.
Why it’s critical: Premedication creates a pharmacological barrier against transient bacteremia. When you perform invasive procedures like extractions or deep scaling, oral bacteria enter the bloodstream. For most patients, the immune system manages this entry without issue. However, for those with specific cardiac vulnerabilities or recent prosthetic implants, these circulating bacteria can colonize damaged heart valves or hardware, leading to life-threatening Infective Endocarditis (IE) or late-stage prosthetic joint infections. Establishing this barrier is a fundamental component of the modern Standard of Care.
Antibiotic Prophylaxis vs. Procedural Sedation
It is vital to distinguish between the various reasons you might premedicate a patient. Antibiotic prophylaxis is strictly a defensive measure for high-risk cardiac subsets. In contrast, procedural sedation involves using anxiolytics, such as benzodiazepines, to manage dental phobia or physiological stress. While their goals differ, their success depends on a shared variable: timing.
- The 60-Minute Window: For maximum efficacy, oral antibiotics must be administered 30 to 60 minutes before the first incision. This ensures peak plasma levels during the period of highest bacteremic risk.
- Sedation Timing: Anxiolytics often require a similar lead time to ensure the patient is sufficiently relaxed before the local anesthetic is administered.
- The Safety Protocol: If a patient forgets their dose, guidelines allow for administration up to two hours post-procedure, though this is a fallback rather than a primary strategy.
Evolution of the ‘Premedicate’ Term in Modern Dentistry
The dental industry has moved away from the “prescribe for everyone” mentality of the 1990s. We’ve entered an era of aggressive antimicrobial stewardship. This shift is driven by the rise of antibiotic-resistant bacteria and the risk of adverse reactions, such as the C. difficile infections associated with clindamycin. Today, to premedicate is to make a targeted, evidence-based decision.
You can no longer rely on a patient’s memory or a surgeon’s vague verbal request. Modern practitioners must justify the decision to prescribe or withhold antibiotics in their clinical notes. This requires clear, vetted communication between the dental office, the patient, and their medical specialists. Standardizing these instructions doesn’t just improve health outcomes; it builds a protective wall around your practice’s reputation. When you replace manual, paper-based tracking with a streamlined digital workflow, you eliminate the friction that leads to missed doses and high-risk misunderstandings.
Clinical Guidelines: Who Needs to Premedicate for Dental Work?
Identifying which patients require antibiotic prophylaxis is a cornerstone of modern patient safety. While historical practices were broad, current standards are increasingly restrictive. The goal is to balance the prevention of rare but severe infections against the very real risks of antibiotic resistance and adverse drug reactions. To premedicate effectively, your team must distinguish between “routine” medical histories and the specific high-risk categories defined by the latest evidence-based protocols.
Why it’s critical: Using antibiotics when they aren’t clinically indicated doesn’t just violate antimicrobial stewardship; it increases your patient’s risk of developing C. difficile or experiencing anaphylaxis. According to the 2021 AHA scientific statement, the shift away from clindamycin was a direct response to these safety concerns. Aligning your office with the current Standard of Care ensures you are protecting both your patient’s health and your practice’s legal standing.
Cardiac Conditions Requiring Prophylaxis
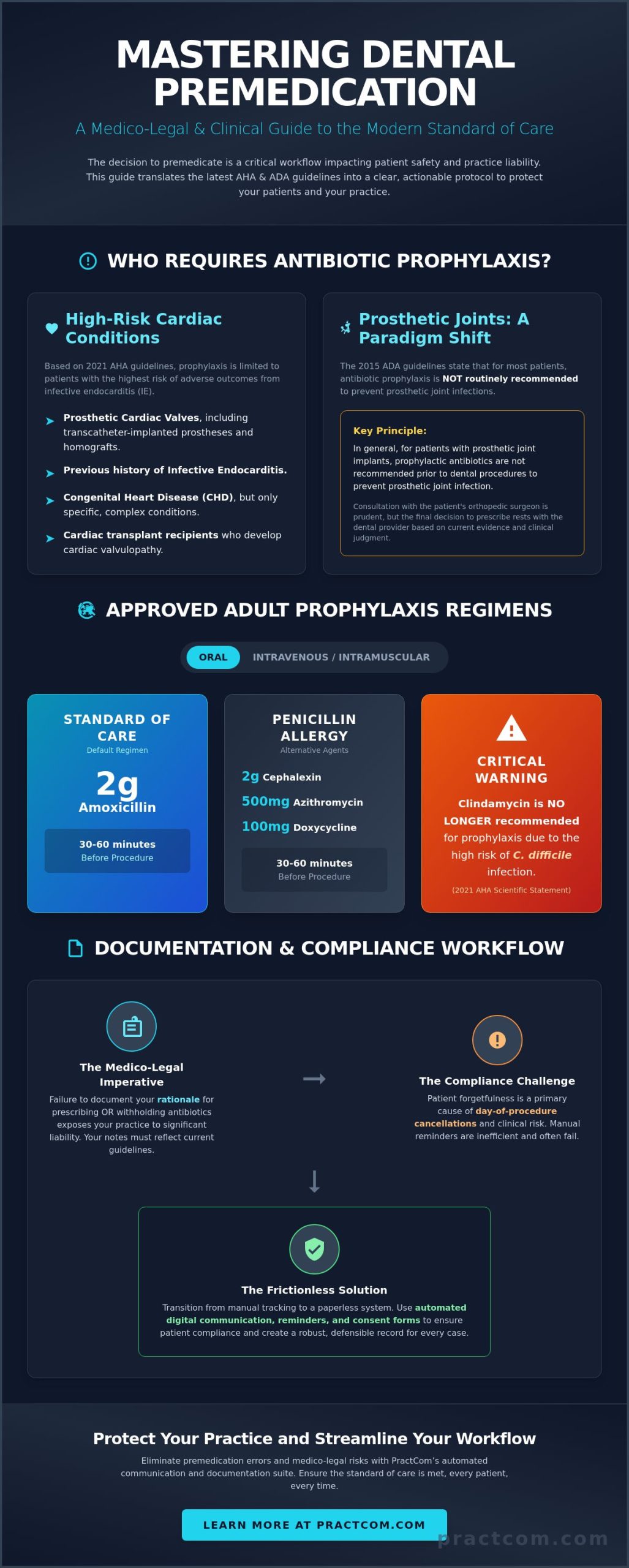
The American Heart Association (AHA) reaffirmed its guidelines in 2021, limiting prophylaxis to a small subset of cardiac patients. This NIH review of premedication protocols highlights that only those at the highest risk for adverse outcomes from Infective Endocarditis (IE) should receive antibiotics. This list currently includes:
- Patients with prosthetic heart valves or those who have used prosthetic material for valve repair.
- Individuals with a prior history of IE, which carries a high mortality rate.
- Specific Congenital Heart Defects (CHD), including unrepaired cyanotic CHD or defects repaired with prosthetic material within the last six months.
- Cardiac transplant recipients who develop heart valve leakage.
Prosthetic Joints and the Orthopedic Consultation
The debate over prosthetic joint premedication remains one of the most common sources of friction in a dental office. The 2015 ADA clinical practice guidelines state that, in general, prophylactic antibiotics are not recommended for patients with prosthetic joint implants. However, many orthopedic surgeons still request that their patients premedicate before any dental intervention. This creates a clinical conflict for the dentist.
When these guidelines clash, the Standard of Care shifts toward a collaborative approach. You should consult the patient’s orthopedic surgeon, especially if the patient has a history of joint complications or is immunocompromised. Documenting this consultation is essential for mitigating liability. To make this process easier, you can use standardized communication templates to quickly request and track these medical clearances. Clear, written recommendations from the specialist provide the medico-legal reassurance your practice needs when guidelines don’t offer a black-and-white answer.
Finally, remember that the procedure itself dictates the risk. Prophylaxis is only indicated for procedures involving significant gingival manipulation or perforation of the oral mucosa. Routine radiographs, placing removable appliances, or shedding primary teeth don’t typically require a pharmacological barrier.
Medico-Legal Importance of Standardized Documentation
Malpractice litigation in dentistry often hinges on a single clinical detail: did the practitioner follow the established Standard of Care? When you instruct a patient to premedicate, you aren’t just giving medical advice; you’re initiating a legal chain of custody. If a patient develops Infective Endocarditis or a prosthetic joint infection following a procedure, your clinical notes become the primary defense against claims of negligence.
Why it’s critical: Documentation must prove that the decision to use or withhold antibiotics was based on current AHA or ADA guidelines. A simple “patient took pre-med” is insufficient. Legal protection requires granular data. You must record the specific antibiotic, the exact dosage (e.g., Amoxicillin 2g), and the timestamp of administration. This level of detail demonstrates that you didn’t just guess; you followed a standardized protocol that prioritized patient safety over administrative convenience.
The Burden of Proof: Clinical Notes and Consent
Relying on verbal confirmation is a significant liability. Patients often misremember timing or dosages. In a courtroom, a patient’s faulty memory can easily outweigh a dentist’s verbal testimony. Paperless dental consent acts as a vetted record that the patient understands both the necessity of the medication and the potential risks, such as allergic reactions or secondary infections. It proves you educated the patient on the risks of non-compliance and the reasons for the specific drug choice. Implementing digital signatures in dentistry takes this protection further by creating a verifiable, timestamped audit trail that proves the informed part of informed consent was genuinely documented and legally sound.
Closing the loop is the final safeguard. Before the procedure begins, the clinical team must verify the medication was taken. If the patient forgot, the incident must be documented. You must record if the procedure was delayed or if the fallback two-hour window was utilized. This final check ensures your practice remains a guardian of patient safety while protecting your professional reputation. It moves your team away from the friction of manual checks toward a standardized system of accountability.
Managing Referrals and Specialist Clearances
When guidelines are ambiguous, such as with certain prosthetic joint cases, the Standard of Care dictates a consultation with the patient’s specialist. A “Request for Clearance” form shouldn’t be a casual note. It needs to be a standardized, trackable document that asks specific clinical questions and receives a formal, written response.
Why it’s critical: A centralized referral system ensures these clearances don’t get lost in a stack of paper or a buried email thread. Having a written recommendation from a cardiologist or orthopedic surgeon shifts the burden of decision-making. It provides a medico-legal shield by showing you performed due diligence. Standardizing this process allows you to premedicate with confidence, moving from administrative chaos to a frictionless, protective workflow that guards your practice’s reputation.
Overcoming Patient Non-Compliance with Premedicate Instructions
A patient arriving for a complex procedure without having taken their antibiotics is a preventable clinical failure. It forces a difficult choice: delay the appointment by an hour, utilize a fallback post-op dose, or cancel the visit entirely. Why it’s critical: every cancelled appointment due to non-compliance represents a direct hit to your practice’s production and wastes valuable chair time that could’ve been allocated to another patient. To premedicate successfully, you must address the psychology of forgetfulness with a system that prioritizes clarity over clinical complexity.
Patients often fail to follow instructions because they don’t understand the “why” or the “when.” When instructions are buried in a packet of paper or delivered in dense medical jargon, the message gets lost. Moving beyond the paper prescription to a digital, plain-language approach ensures the protocol is impossible to ignore. It transforms a passive instruction into an active, trackable workflow that guards your schedule and your patient’s health.
Designing Frictionless Pre-Op Instructions
Effective communication starts with simplicity. Your instructions should be written at a 5th-grade reading level to ensure total comprehension across your entire patient base. Instead of using terms like “antibiotic prophylaxis,” use direct, actionable language: “Take your 4 blue pills 1 hour before your appointment time.” This reduces the cognitive load on the patient and minimizes the chance of error. You can achieve this level of clarity without adding friction to your day by using a standardized communication suite to send these instructions via SMS or email in seconds.
- Five-Click Delivery: Standardize your workflow so the team can send vetted instructions instantly during the treatment planning phase.
- Multi-Language Support: Ensure your non-English speaking patients receive the protocol in their native language to eliminate translation errors.
- Visual Cues: Digital templates can include bolded text or specific icons to emphasize the critical 60-minute window.
Automated Reminders and Verification
Your front desk team is already stretched thin. Manually calling every patient to verify they have their medication is an inefficient use of resources. Automated “T-minus 24 hour” alerts act as a pre-emptive strike against forgetfulness. These reminders don’t just tell the patient what to do; they ask for verification. A patient portal allows the patient to click a button to confirm they have their prescription ready and understand the timing. This provides the peace of mind your clinical team needs before the patient even walks through the door.
Standardizing this verification loop ensures the Standard of Care is met for every case. When the system handles the follow-up, your team can focus on high-value clinical tasks rather than chasing down compliance. It creates a controlled environment where “I forgot” is no longer a standard part of your morning huddle. By automating the mundane, you ensure that the instruction to premedicate is followed with 100% accuracy, protecting both the patient’s heart and your practice’s bottom line.
Streamlining Your Workflow with PractCom’s Communication Suite
Managing the instruction to premedicate shouldn’t be a source of daily stress for your clinical team. While the clinical guidelines from the AHA and ADA provide the framework, PractCom provides the execution engine. Our library features over 80 vetted templates designed specifically to bridge the gap between complex medical requirements and patient understanding. By moving these protocols into a centralized system, you replace the chaos of manual tracking with the control of an automated workflow. You can finally stop relying on sticky notes and verbal reminders that often lead to clinical friction.
Why it’s critical: Automated systems ensure no patient “falls through the cracks” because a physical referral card was lost or a verbal instruction was forgotten. This isn’t just about administrative speed; it’s about safeguarding the Standard of Care across every operatory in your practice. When your team uses a standardized system, you eliminate the variability that leads to medico-legal vulnerability. You move from a reactive posture to a proactive one, ensuring every high-risk patient is prepared before they ever sit in your chair.
Digital Consent and Instruction Integration
PractCom allows you to link premedication instructions directly to the paperless dental consent form. This integration creates a frictionless experience for the patient and a robust medico-legal audit trail for the practice. Every time a document is sent, opened, or signed, the system logs the activity with a precise timestamp. This digital paper trail is your first line of defense in malpractice prevention.
You no longer have to wonder if a patient received their pre-op protocol. The tracking logs provide the definitive proof required to mitigate liability in the event of a complication. Your clinical team can deliver these materials with a One-Click template delivery system, ensuring they spend more time with patients and less time on repetitive administrative tasks. It’s a system designed by those who understand the physical and mental demands of a busy dental office.
Scaling the Standard of Care Across Your Practice
Consistency is the ultimate protection against clinical errors. When you have multiple providers or locations, ensuring every team member follows the same 2026 antibiotic regimens is a significant challenge. PractCom standardizes these interactions by providing a single source of truth for your entire team. Whether it’s a standard prophylaxis or a complex orthopedic consultation, the protocol remains uniform and vetted.
You can use the Performance Dashboard to monitor how patients engage with your pre-op materials in real-time. If a specific patient hasn’t opened their instructions 48 hours before their scheduled surgery, your team can intervene early. This proactive approach transforms a clinical necessity into a high-level administrative efficiency that protects your production schedule and your peace of mind. Ready to eliminate the friction from your daily schedule? Standardize your premedication protocols with PractCom and protect your practice’s reputation today.
Secure Your Practice and Elevate Patient Care
You now have the tools to navigate the evolving landscape of dental prophylaxis with confidence. By aligning your office with evidence-based standards, you move from clinical guesswork to professional certainty. Why it’s critical: having a consistent, documented protocol to premedicate high-risk patients is the only way to satisfy the modern Standard of Care. It protects your patients from systemic infection and shields your practice from the anxiety of potential litigation.
Standardizing these workflows shouldn’t add friction to your day. PractCom offers a library of 80+ vetted clinical templates that simplify complex instructions into plain language. With multi-language support in 15 languages and automated medico-legal audit trails, you can verify compliance without chasing down every patient. This level of control replaces administrative chaos with a streamlined, One-Click system that functions even when your team is stretched thin. Take the next step toward a more secure and efficient operatory. Streamline your clinical documentation with PractCom’s instruction library and gain the peace of mind that comes with a standardized workflow. Your practice deserves the protection of a reliable clinical ally.
Frequently Asked Questions
Does a patient need to premedicate for a simple dental cleaning?
Yes, if the patient falls into the high-risk cardiac categories defined by the 2021 AHA guidelines. Prophylaxis is required for any procedure involving gingival manipulation or perforation of the oral mucosa. This includes subgingival scaling and professional cleanings where bleeding is anticipated. Why it’s critical: bacteria can enter the bloodstream even during routine hygiene, making a pharmacological barrier necessary for vulnerable patients.
What happens if a patient forgets to premedicate before their appointment?
If a patient forgets their dose, the antibiotic can be administered up to two hours after the dental procedure. However, the preferred protocol is to administer the medication in the office and wait 30 to 60 minutes before starting treatment. If this delay isn’t possible, you may need to reschedule the appointment to avoid clinical risks and maintain your practice’s Standard of Care.
Can a dentist prescribe the premedication, or must it come from a specialist?
A dentist can absolutely write the prescription, though it’s often based on a recommendation from the patient’s cardiologist or orthopedic surgeon. The key is to premedicate based on a clear, documented medical necessity. You should maintain a written record of the specialist’s clearance in the patient’s digital chart to provide a robust medico-legal audit trail and ensure all providers are aligned.
What are the common antibiotics used to premedicate for dental procedures?
The standard regimen for adults is 2g of Amoxicillin taken orally. If the patient is unable to take oral medications, 2g of Ampicillin or Cefazolin administered IV/IM is the common alternative. Why it’s critical: since the 2021 AHA update, clindamycin is no longer recommended due to the high risk of C. difficile infections and severe adverse reactions.
Is premedication still required for patients with total joint replacements in 2026?
Generally, the 2015 ADA guidelines state that antibiotics are not recommended for patients with prosthetic joint implants. However, the Standard of Care often involves a collaborative decision between the dentist and the orthopedic surgeon. If the surgeon recommends that a patient should premedicate due to a history of joint complications, you should follow that recommendation and document the consultation thoroughly.
How long before the dental procedure should a patient take their premedication?
Patients should take their medication 30 to 60 minutes before the procedure begins. This timing ensures that the antibiotic reaches peak plasma levels in the bloodstream at the exact moment the oral mucosa is manipulated. Standardizing this instruction through automated reminders helps prevent the scheduling friction caused by patients who take their medication too late or forget it entirely.
Are there alternatives for patients who are allergic to penicillin and need to premedicate?
For patients with penicillin allergies, the recommended alternatives include 2g of Cephalexin, 500mg of Azithromycin or Clarithromycin, or 100mg of Doxycycline. Cephalexin should only be used if the patient’s allergic reaction was not anaphylaxis. Clindamycin was removed from these alternative options in 2021 to improve patient safety and reduce the risk of secondary infections.
Can a patient premedicate with over-the-counter medications for dental anxiety?
No, over-the-counter medications are not a substitute for professional procedural sedation. While some patients may try to use antihistamines or herbal supplements, these aren’t standardized for clinical use in a dental setting. Any medication used to manage anxiety must be prescribed and monitored by the clinician to ensure it doesn’t interfere with local anesthetics or other prescribed antibiotics.

Article by
Cary Ganz DDS
Dr. Cary H. Ganz is a dentist, prosthodontist, entrepreneur, lecturer, and author with more than 50 years of experience in clinical dentistry and dental technology. Throughout his career, he has combined hands-on patient care with a deep understanding of how technology can improve dental practice operations, communication, documentation, and patient outcomes.
In addition to his clinical background, Dr. Ganz has held significant leadership roles in the dental technology industry, including Past Owner and Vice President of Clinical Affairs at DEXIS Digital Radiography and Past Vice President of Clinical Affairs at Denticon Practice Management Software. His business experience includes product development, clinical strategy, dental software innovation, practice management solutions, and educating dental professionals on the effective use of technology in modern dentistry.
Today, Dr. Ganz continues to focus on creating practical technology solutions for dental practices, including PractCom, a comprehensive dental practice communication platform designed to improve patient communication, documentation, compliance support, referrals, and overall practice efficiency. His work reflects a career-long commitment to helping dentists deliver better care while making their practices more organized, efficient, and protected.
No responses yet